IMT Ultrasound Imaging
Chapter 17
Chapter 17: IMT Ultrasound Imaging
469
17
Background
The concept for measuring intima-media thickness (IMT) was
first introduced by Paolo Pignoli, M.D., et. al., in the AHA journal
Circulation
, in 1986. Pignoli purported for the first time that
“B-mode imaging represents a useful approach for themeasurement
of intimal and medial thickness of human arteries in vivo.”
1
The
foundational concept is that the characteristic B-mode appearance
of the abdominal aortic wall could serve as an indicator of plaque
burden, or systemic atherosclerotic load. Since atherosclerosis is
well known to be a progressive and systemic process, it is believed
that atherosclerosis found in the larger arteries, such as near the
carotid bifurcation,correlates well with the disease progression that
occurs within coronary and cerebrovascular arterial trees. Therefore,
the early stages of atherosclerosis can be assessed in the relatively
easily imaged vessels of the arterial system (such as the common
carotid artery), yielding valuable information regarding the much
more challenging-to-image coronary artery system. In essence, an
individual’s carotid IMT (CIMT) measurement is compared with
accepted“normal ranges” (normative values) to determine a risk of
coronary artery disease and cardiovascular risk.
Shortly after Pignoli’s publication,a prolific series of IMT studies be-
gan called
Atherosclerosis Risk in Communities
(ARIC),the data from
which are often cited today as normative measurements in patients
45 to 65 years old. There are now a number of consensus papers
on applying CIMT to risk stratification (including: the
Prevention
ConferenceV published in Circulation
2002,the important
Mannheim
Intima-Media Thickness Consensus
published in Cerebrovascular
Diseases in 2004, and more recently
A Consensus Statement from
the American Society of Echocardiography Carotid Intima-Media
Thickness Task Force
from Stein et. al. published in
JASE
in 2008).
Hundreds of publications have described CIMT as it relates to lipid
metabolism and relative risk for atherosclerosis-mediated clinical
events. CIMT has evolved into a well-validated and respected tool
in both research and clinical settings as a measure of atherosclerotic
burden.This coupled with the relatively low expense,ease of use,and
absence of ionizing radiation implies a likely increase in application
of ultrasound-based IMT exams in the future.
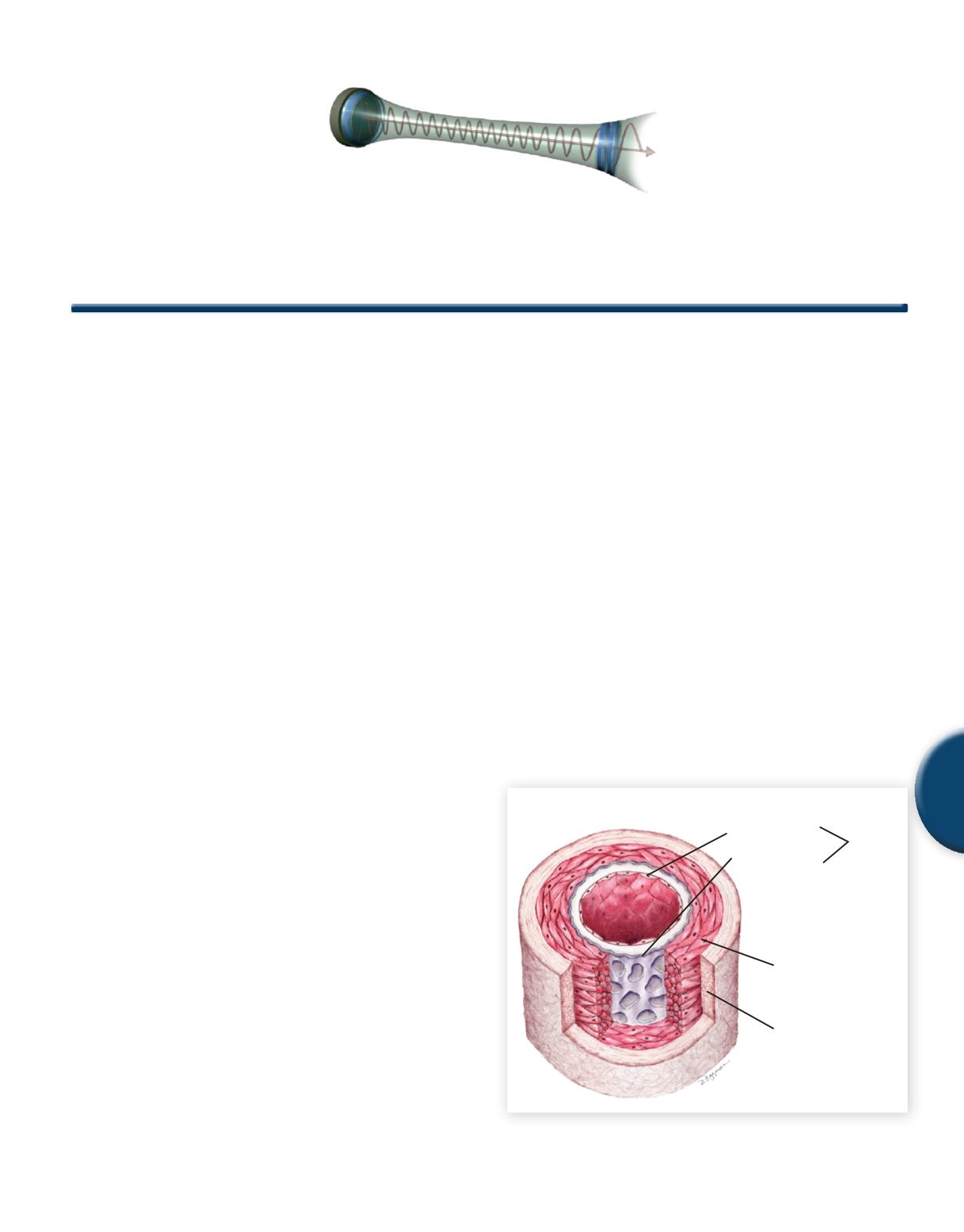
1. Carotid Artery Anatomy
To understand the specific techniques and required ultrasound
system manipulation to acquire accurate IMT measurements, it is
important to understand arterial anatomy. The carotid artery, like
all large arteries in the human body, is architecturally arranged in
three concentric layers (
Figure 1
). The innermost layer, the tunica
intima, is merely a single layer of endothelial cells supported by
a thin sub-endothelial elastic lamina. The tunica media is much
thicker, consisting of a dense fibromuscular layer. The outermost
layer, the tunica adventitia is a less-dense network of supporting
connective tissue, primarily collagen matrix. These three layers, in
concert with the blood pool in the artery lumen, create a distinct
and reproducible signature on B-mode ultrasound, particularly
when imaged in the longitudinal plane. Two distinct lines are vis-
ible in the signature corresponding with the blood-intima boundary,
and the intima-media boundary. At these histological boundaries
the respective tissue densities differ, resulting in different acoustic
impedances. The mismatch between these acoustic impedances
produces relatively strong ultrasound reflections,accounting for the
easily visualized bright-dark-bright telltale signature of the CIMT
complex (as shown in
Figure 2
).
endothelium
internal elastic
membrane
tunica
intima
tunica media
tunica adventita
Fig. 1
Three concentric layers of an artery
David Parlato, BA, RVT


