Chapter 18: Speckle Tracking and Cardiac Strain
479
18
1. Introduction and Definition of Strain and
Strain Rate
1.1 The Need for Cardiac Deformation Imaging
Many forms of heart disease result in heart failure. Ultimately per-
manent damage in muscle fibers through cardiomyopathy results
from many causes. Temporary ischemia can cause reductions in
wall motion and hence reduce myocardial strain. Additionally, che-
motherapy can poison healthy heart muscle cells as well as targeted
cancer cells - this also can reduce myocardial strain. The ability
to distinguish sound heart muscle from damaged heart muscle is
important for determining correct diagnosis and treatment. By
analyzing wall motion, heart muscle viability can be assessed uti-
lizing various ultrasound technologies. Wall motion can be more
objectively analyzed using computer-based techniques, such as
speckle tracking, instead of the human eye.
1.2 CardiacMechanics: Translation, Rotation, andTorsion
One of the challenges of measuring cardiac deformation is the com-
plexmotion of the heart,including translation,rotation,and torsion.
Before addressing assessment of cardiac wall motion,it is important
to first understand different forms of motion. Translation represents
rigid motion of a body. For example, if a coffee mug slides across
a table without “turning,” the cup has been translated. If the cup is
turned, whether or not the cup has undergone translation, the cup
has undergone“rotation.” In this case,the axis of rotation runs from
the table through the top of the cup. When we consider rotation of
the heart, we usually imagine a longitudinal axis running from the
apex through the center of the mitral valve.
In a SAX view, the normal myocardium undergoes rotation (e.g.
basal level). At another level (e.g.apex),the myocardiumundergoes
rotation but differently. The distinction in rotation fromone level to
another accounted for by the long-axis length between planes de-
notes“torsion”similar to the wringing of a towel. The heart consists
of helical fibers so that it actually “twists” as it contracts. Torsion
and rotation are not routine clinical measurements.
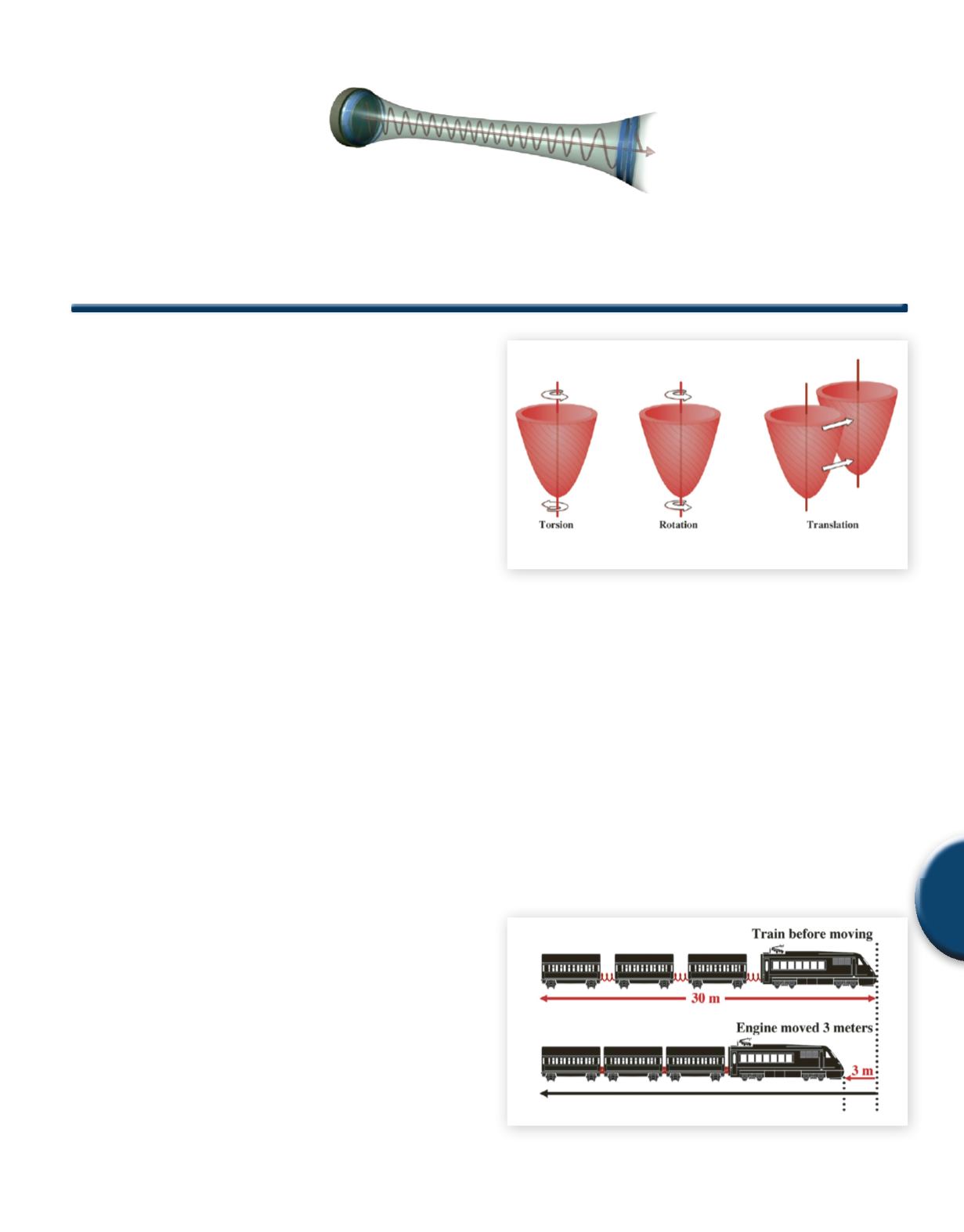
Fig. 1
Cardiac motion
1.3 Strain
To analyze cardiac tissue, one approach is to measure strain. Strain
is simply a percentage change in length. Tension represents forces
that tend to elongate tissue whereas compression tends to shrink
tissue. Since longitudinally oriented fibers shorten, normal strain
is negative as is circumferential strain. However, the normal myo-
cardium thickens during systole so radial strain is typically positive.
The rest length in diastole is used for reference in the calculations
of strain. Note that strain is a dimensionless number and hence,
has no units. It is simply determined as a percentage change. This
concept is illustrated by the following example inwhich a train starts
to back up. In this case notice that the total length of the train is
compressed by 3 meters from the original 30 meters. As such this
would indicate a negative strain of 10% (-3m/30m).
Fig. 2
A strain of negative ten percent
Ivan S Salgo, MD, MS; Chief, Cardiovascular Investigation; Research & Development, Ultrasound; Philips Healthcare
Speckle Tracking andCardiac Strain
Chapter 18


